
Enterobius vermicularis is an intestinal nematode of humans and is especially prevalent among children. It is widely distributed throughout the world, even in developed countries. Normally it lives in the cecum and migrates out through the anus for oviposition. Since it is a lumen-dweller, its infection is not medically serious, but it can be troublesome on rare occasions when the worm invades tissue. The commonest site of tissue invasion is the mucosa and submucosa of the appendix and the next commonest is the female genital tract (Beaver et al., 1984). The female genital tract is the most frequent site of extraintestinal parasitism of E. vermicularis because the worm often migrates into the vagina and invades the uterus, uterine tube, ovary, and even the peritoneum (Saffos and Rhatigan, 1976; Beckman and Holland, 1981). In addition, rarely it has been reported to form a granuloma in the perineum (Kim and Chi, 2000), the lung (Beaver et al., 1973), and the liver (Little et al., 1973).
When the worm invades tissue it dies within a few days and then degenerates, but its eggs may remain longer. Eggs in tissue may be helpful for diagnosis due to the longevity of the eggshell. We describe briefly a human case of ovarian enterobiasis, which was diagnosed on basis of egg morphology.
A 36-year old woman visited the gynecology clinic of the Seoul Asan Medical Center on 12 June 2001 for the further evaluation of a known pelvic mass. She had previously consulted a private clinic for a regular gynecological examination on 30 May 2001, and had been informed of a cystic mass of 13 cm diameter at her right ovary. Transvaginal ultrasonography revealed a huge pelvic mass of 11.9 × 10.1 × 10.7 cm with a solid and a nodular inner portion. Under the impression of ovarian cancer she received total abdominal hysterectomy, bilateral salpingoophorectomy and omentectomy with a selective pelvic lymph node biopsy on 18 June 2001.
The resected specimen consisted of two ovaries and tubes, uterus, omentum and lymph nodes. The left cystic ovary (12 × 12 × 11 cm, 657 g) with attached fallopian tube (3 cm in length and 0.4 cm in diameter) appeared smooth on its external surface, and the unilocular cyst was found to contain mucoid material. However, the internal surface showed multiple grape-like projections, which measured 6.5 × 6 × 1.8 cm. The cut surface of the projections glistened and was yellowish white in color. The remaining cystic wall had a maximum thickness of 0.5 cm, and showed neither hemorrhage nor necrosis. The fallopian tube was unremarkable.
The right ovary was a grape-like mass (6.5 × 4 × 2 cm and 19 g) and the fallopian tube was 7 cm in length and 0.9 cm in diameter. An aggregate of papillary masses (4.5 × 2.2 × 2 cm in total) was present on the serosal surface of the right ovary. The remaining ovarian parenchyma was unremarkable as was the fallopian tube.
The uterus was symmetric with attached pericervical fat tissue (10 × 7.5 × 4 cm, 146 g). The serosal surface of the uterus was pinkish, focally eroded and hemorrhagic. No definite mass lesion was seen in the uterine serosa. The myometrium and endometrium measured 2.2 and 0.2 cm in thickness respectively. The cervix was unremarkable but the pericervical tissue contained a well-demarcated nodule (1.5 × 1 × 1 cm).
The omentum weighed 160 g and contained no mass. The pelvic lymph nodes were three aggregates of the yellowish fibroadipose tissue, measuring up to 4 × 3 × 1.5 cm.
Histopathological diagnosis was of a borderline serous neoplasm with micropapillary features of the left and right ovary with pericervical invasive implant. The endometrium was in the proliferative phase and the cervix showed chronic inflammation and squamous metaplasia.
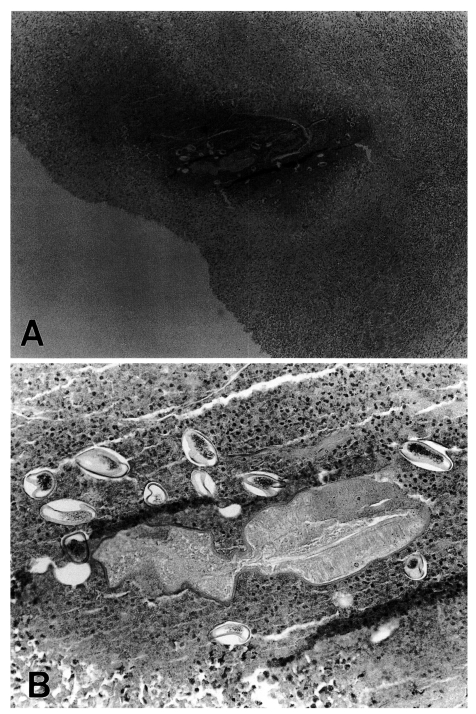
In the left ovary, a necrotic focus was found in the parenchyma, and this was surrounded by granulation tissue. A section of a nematode was observed in the center of the necrotic tissue and several eggs were scattered around the worm section (Fig. 1A). The sectioned worm had a thick cuticular surface but the other structures had degenerated and were thus difficult to identify (Fig. 1B). The body diameter measured 600-800 µm. Several eggs were observed amongst the inflammatory cells surrounding the worm (Fig. 1B). Eggs included a germ in the thick chitin shell (Fig. 1B), and measured 56-60 × 27-30 µm with one convex side. The size and shape of the eggs identified them as belonging to E. vermicularis.
Ovarian enterobiasis is rare but several cases have been recorded (Beckman and Holland, 1981). The uterine tubes and peritoneal serosa are common sites of ectopic enterobiasis. The majority of the cases have reported symptom of abdominal pain. All of the cases have been identified by surgical biopsy of the involved organs. The present case showed no specific subjective symptoms related with ovarian enterobiasis probably because of coincidental ovarian cancer. Ovarian enterobiasis is rare but it still occurs in Korea.